
Today we saw some great cases:


2. High Estrogen states associated with liver disease, look for:
3. For underlying clues as to the etiology of liver disease, look for:
Below: duputrene's contracture, palmar erythema, and spider angioma





2. Eruptive xanthoma: can be pruritic, and may resolve over a few weeks. Often seen in patients with diabetes and hyperlipidemia. Pustular on an erythematous base.
3. Tendon xanthoma: classically a slowly appearing nodule on the extensor tendons of hands and feet.
4. Lipemia retinalis: Very high levels of triglycerides (>400 in the USA, >40 in the rest of the world). You can see a milky colouration to the retinal vessels.
A neat link from NEJM on lipemia retinalis over here.
 On inspection remember to look for "SEADS" - swelling, erythema, atrophy, deformities, skin changes.
On inspection remember to look for "SEADS" - swelling, erythema, atrophy, deformities, skin changes.Hand:
Fingers:


Cranial Nerve IV
Cranial Nerve VI
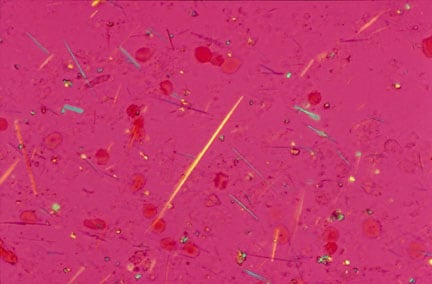
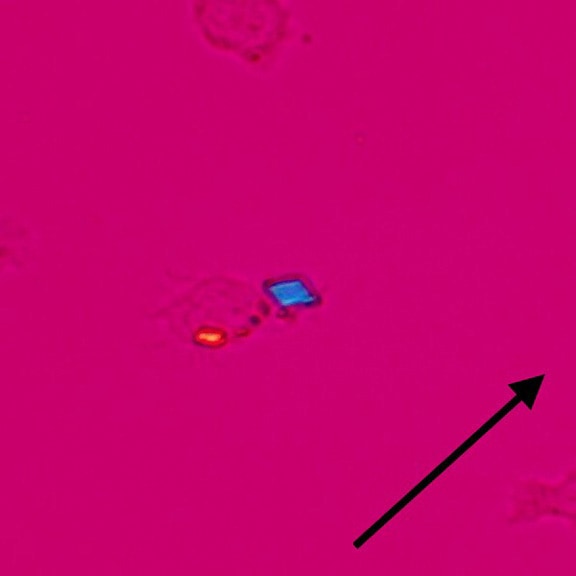
 Today we saw some pretty empressive gouty tophi - small joints on the hands were involved, as well as an impressive tophus on the elbow (this picture is from wikipedia, not our patient). Tophi are just uric acid crystals deposited in the tissues, and is evident usually after several years of gout. Remember to look for tophi on the joints, but also in the helix/antihelix of the ear (see picture below).
Today we saw some pretty empressive gouty tophi - small joints on the hands were involved, as well as an impressive tophus on the elbow (this picture is from wikipedia, not our patient). Tophi are just uric acid crystals deposited in the tissues, and is evident usually after several years of gout. Remember to look for tophi on the joints, but also in the helix/antihelix of the ear (see picture below). Tophi on the ear
 -Tunisia?
-Tunisia?Let me know if you need this explained again at the bedside - happy to show you at any time.
3. Links:



{kind=link}
{kind=link}