 Today we saw some pretty empressive gouty tophi - small joints on the hands were involved, as well as an impressive tophus on the elbow (this picture is from wikipedia, not our patient). Tophi are just uric acid crystals deposited in the tissues, and is evident usually after several years of gout. Remember to look for tophi on the joints, but also in the helix/antihelix of the ear (see picture below).
Today we saw some pretty empressive gouty tophi - small joints on the hands were involved, as well as an impressive tophus on the elbow (this picture is from wikipedia, not our patient). Tophi are just uric acid crystals deposited in the tissues, and is evident usually after several years of gout. Remember to look for tophi on the joints, but also in the helix/antihelix of the ear (see picture below). Gout:
- Clinical: Typically presents with acute monoarthritis, occasionally a few joints involved. Red, hot, swollen, tender. Often first MTP, ankle, knee.
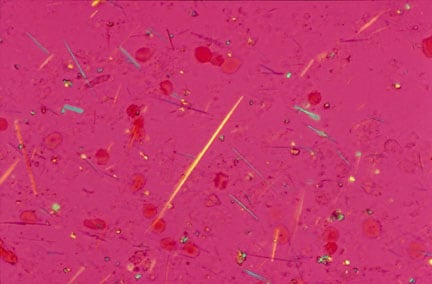
- Evaluation: Negatively birefringent crystals visualized, often intracellular. They look like this. These are monosodium urate crystals.
- Risk factors: hyperuricemia (lymphoma, other causes of increased cell turnover), obesity, EtOH, medications like HCTZ, asa.
- Acute Treatment: NSAIDS, intra-articular steroids, colchicine, systemic steroids if multiple joints involved.
- Chronic treatment: Allopurinol if multiple attacks per year (usually >2).
Pseudo Gout:
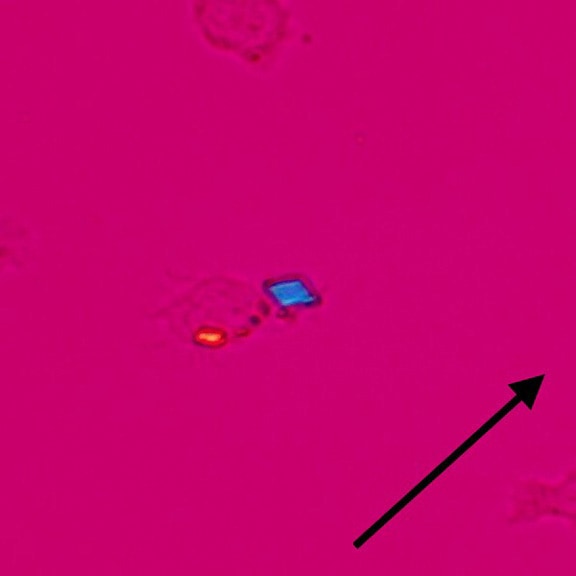
- Rhomboid crystals, occasionally inside macrophages. They look like this. These are calcium pyrophosphate crystals.
- Often in elderly patients with multiple medical problems.
- Often polyarticular, and may affect wrists, shoulders.
Tophi on the ear








 Today we saw some really interesting cases including:
Today we saw some really interesting cases including:


{kind=link}
{kind=link}