
Today we saw some great cases:


2. High Estrogen states associated with liver disease, look for:
3. For underlying clues as to the etiology of liver disease, look for:
Below: duputrene's contracture, palmar erythema, and spider angioma





2. Eruptive xanthoma: can be pruritic, and may resolve over a few weeks. Often seen in patients with diabetes and hyperlipidemia. Pustular on an erythematous base.
3. Tendon xanthoma: classically a slowly appearing nodule on the extensor tendons of hands and feet.
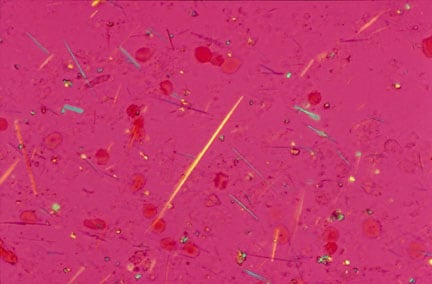
4. Lipemia retinalis: Very high levels of triglycerides (>400 in the USA, >40 in the rest of the world). You can see a milky colouration to the retinal vessels.
A neat link from NEJM on lipemia retinalis over here.
 On inspection remember to look for "SEADS" - swelling, erythema, atrophy, deformities, skin changes.
On inspection remember to look for "SEADS" - swelling, erythema, atrophy, deformities, skin changes.Hand:
Fingers:


Cranial Nerve IV
Cranial Nerve VI
 Today we saw some pretty empressive gouty tophi - small joints on the hands were involved, as well as an impressive tophus on the elbow (this picture is from wikipedia, not our patient). Tophi are just uric acid crystals deposited in the tissues, and is evident usually after several years of gout. Remember to look for tophi on the joints, but also in the helix/antihelix of the ear (see picture below).
Today we saw some pretty empressive gouty tophi - small joints on the hands were involved, as well as an impressive tophus on the elbow (this picture is from wikipedia, not our patient). Tophi are just uric acid crystals deposited in the tissues, and is evident usually after several years of gout. Remember to look for tophi on the joints, but also in the helix/antihelix of the ear (see picture below). Tophi on the ear
 -Tunisia?
-Tunisia?Let me know if you need this explained again at the bedside - happy to show you at any time.
3. Links:



 What does this picture have to do with splenomegaly? Send me an email - if you're right, I'll buy you a coke.
What does this picture have to do with splenomegaly? Send me an email - if you're right, I'll buy you a coke. 
 Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis are about as bad a drug reaction as you can get. These are basically the same condition, with TEN being on the more serious side of the spectrum compared to SJS
Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis are about as bad a drug reaction as you can get. These are basically the same condition, with TEN being on the more serious side of the spectrum compared to SJS Today we looked at nails a bit more closely. We examined the white part of the nail, termed the Lunula, which is Latin for 'little moon'. This normally occupies a very small proportion of your nail.
Today we looked at nails a bit more closely. We examined the white part of the nail, termed the Lunula, which is Latin for 'little moon'. This normally occupies a very small proportion of your nail. Today we saw some really interesting cases including:
Today we saw some really interesting cases including:*Clubbing: also discussed, with evidence-based exam findings at this link.
One patient we saw had terrible interstitial lung disease. These are confusing conditions. Here's an approach as to the underlying etiology:
Systemic Diseases: ILD is found commonly in Sarcoidosis and Collegen Vascular Diseases - the prototype being Scleroderma. Remember, ILD is not so common in SLE or Rheumatoid arthritis.
Exposures: these are classically divided into organic and inorganic exposures:

Physical Examination for clubbing:
What is the evidence for all this?
 Today we saw of case of severe non-pitting edema, and a case of what appeared to be cellulitis, but in fact was radiation-induced skin changes.
Today we saw of case of severe non-pitting edema, and a case of what appeared to be cellulitis, but in fact was radiation-induced skin changes.Unilateral Edema: this may be caused by


So what are the "Associated Findings"?

These symptoms may start abruptly and develop over a period of hours, days, to a couple of weeks.
A related variant: the Miller-Fischer Syndrome: This is under the same umbrella as GBS and is manifested by 1. Ophthalmoplegia, 2. Ataxia, 3. Areflexia. Patients will also usually have peripheral weakness.
Diagnosis: You will hear the term "Albuminocytologic Dissociation". This means that in the CSF there are elevated protein levels with normal WBC counts. This is a classic feature of GBS. Nerve conduction studies will also help clinch the diagnosis. MRI will often show enhancement of nerve roots.
Treatment: with plasma exchange or IVIG therapy. This is to eliminate or incapacitate auto-antibodies to schwann cells. Patients must be watched closely for possible respiratory muscle compromise. Roughly 80% will make a full recovery.
Risk Factors: Autoantibodies may form after exposure/infection:
A few good links:
 Mitral Regurgitation is pretty common. when you hear this murmur and are trying to determine the underlying cause, think about the individual components of the mitral valve and particular disease states which might affect them. Let's start at the annulus and work our way down....
Mitral Regurgitation is pretty common. when you hear this murmur and are trying to determine the underlying cause, think about the individual components of the mitral valve and particular disease states which might affect them. Let's start at the annulus and work our way down....Good Links:
 (a leaky valve, pictured left)
(a leaky valve, pictured left)Aortic Insufficiency: probably the most eponymous physical exam scenario....
Etiology of Aortic Insufficiency:
What's with all the eponyms? These are cool to see, but largely useless as they are not sensitive or specific, and are mostly related to the wide pulse pressure.
So, is there any evidence for all this?
A little bit. Some smart folks in Toronto wrote a good JAMA article that you can read at this link. AI can be ruled out with the absence of an early diastolic murmur, and ruled in with the presence of an early diastolic murmur - the caveat? These murmurs were heard by cardiologists. Perhaps mere mortals like ourselves will hear it too.


*A good way to test for proximal muscle weakness in this condition is to have a person sit in a chair with their arms folded across their chest, and have them attempt to stand up.
*Remember that many patients with Dermatomyositis have an underlying malignancy, and the diagnosis of Dermatomyositis should prompt an age-appropriate and risk-factor-appropriate malignancy screen. This link shows some new data relating the two conditions.
(periungual vascular changes pictured left)
 (telangiectasia pictured left)
(telangiectasia pictured left)
CREST Syndrome:
Here is a good link to a review on Scleroderma.

(sclerodactyly pictured left)






 An aerial view of the Hoover dam pictured left.
An aerial view of the Hoover dam pictured left.Aortic Stenosis. Know it. Love it. You will see it every day on the wards and in clinic.
Pathogenesis of Symptoms: large afterload leads to concentric left ventricular hypertrophy à high oxygen demand and ischemia (especially in subendocardium) à decreased compliance à fixed time of systole so when HR is high then diastole too short to fill ventricle àeventually leads to LV failure.

A word on sarcoid - we touched on the two acute manifestations of this condition:


{kind=link}
{kind=link}
{kind=link}